

ECOG performance status (ECOG; Oken, 1982) is a unidimensional tool that does not measure independently patient general condition prior to diagnosis (Dx) and may modified by pre-phase therapy (Rx). Multidimensional evaluation of patient general condition is currently recommended by NCCN, ASCO and EORTC in elderly patients with cancer, commonly used as a predictor of life-expectancy and as a tool for detecting and palliate any underlying deficits. Treatment tolerability (TOL) can be predicted in patients with solid neoplasms by dedicated tools such as CARG (Hurria, 2011) and CRASH (Extermann, 2012), but they are not readily applicable to hematologic malignancies because these neoplasms, and the most commonly used therapeutic schemas in this group of diseases, have not been part of their clinical development.
Our study aims to analyze the eventual association between TOL and the categories of commonly used multidimensional scales, such as the Geriatric Assessment in Hematology (GAH; Bonanad, 2015) and the Lee Index for Older Adults (LEE; Lee, 2006), in elderly patients receiving first-line immuno/chemotherapy.
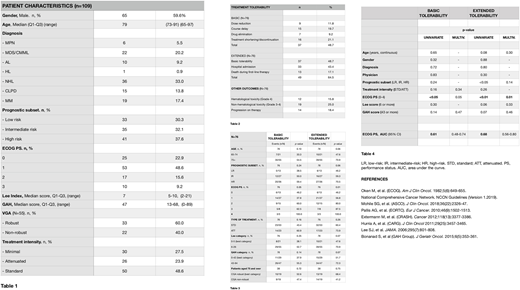
We have analyzed a prospective cohort of 182 adult patients diagnosed with hematologic malignancies in our center during the calendar year 2008. All patients gave written informed consent and the study was approved by our IRB. One hundred nine patients were older than 65 years and had their chart reviewed and general condition evaluated by ECOG, GAH and LEE (Table 1). Those aged 75 and over also received a Comprehensive Geriatric Assessment and were categorized as robust or non-robust. Seventy nine received immuno/chemotherapy (standard 53, attenuated 26) while 30 patients received only minimal Rx (supportive care or watch & wait). TOL was defined as the ability to receive Rx without modifications and measured by 2 composite endpoints: 'basic' and 'extended' TOL. Basic TOL included either: 1) dose reduction, 2) course delay, 3) drug elimination, or 4) Rx shortening/discontinuation not due to progressive disease; extended TOL also included 2 additional items, namely, 5) non-programmed hospital admission or 6) death during the first-line Rx. We followed standard statistical procedures including stepwise logistic regression, adjusting for 1) age (continuous), 2) gender, 3) diagnostic group, 4) physician, 5) prognostic subset (favorable, intermediate or unfavorable) specific for each diagnostic group, 6) ECOG (0-4) and 7) Rx type (standard vs attenuated). GAH and LEE scores were dichotomized following commonly used cutoffs in the clinic (GAH 0-42 vs 43-94; LEE 0-5 vs 6-26).
Basic TOL was inadequate in 48.7%, and extended TOL in 64.5% of the patients (Table 2). We did not find any statistical association (Table 2) between basic/extended TOL and either GAH or LEE categories (cutoff 43 and 6, respectively). The only covariate that a statistically significant association to both basic and extended TOL was ECOG (Table 3). Multivariate analysis confirmed the association between ECOG and TOL (basic; p=0.05; extended, p=0.01) as well as the lack of association of TOL with GAH or LEE categories (Table 4). ROC analysis showed that ECOG score (0-4) explains 61% of the observed variability of basic TOL (AUC 95% CI 0.48-0.74) and 68% of extended TOL (AUC 95% CI 0.56-0.80). In addition, Comprehensive Geriatric Assessment stratification (robust vs non-robust) was not associated to TOL in the patients older than 75.
In summary, we have observed no statistically significant association between treatment tolerability and the categories of Geriatric Assessment in Hematology or Lee Index for Older Adults. By contrary, ECOG was associated to that endpoints in the wide spectrum of hematologic malignancies.
Ramos:Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees, Other: travel and research grants; Novartis: Consultancy, Other: travel grant; Amgen: Consultancy, Other: travel grant; Abbvie: Consultancy, Other: travel grant; Jannsen: Other: travel grant; Roche: Other: travel grant; Rovi: Other: travel grant; Merck-Sahrp & Dohme: Other: travel grant; Daiichi-Sankyo: Other: travel grant; Takeda: Consultancy, Other: travel grant .

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal